The Mortality Census
The coroner’s office has a long, deep history, stretching back to the Middle Ages and forward to the present. The mortality census, by contrast, was the short-lived product of a peculiar place and time. Obviously, the census itself is baked into the United States Constitution as a requisite of representative government. Article I first creates Congress and then notes that “Representatives and direct Taxes shall be apportioned among the several States ... according to their respective Numbers.... The actual Enumeration shall be made within three Years after [1787] ... and within every subsequent Term of ten Years.” Strictly speaking the only Constitutionally required function of the census is to count heads for the purpose of apportioning representatives to Congress and the Electoral College, and if that was all the census ever did the screenwriter Aaron Sorkin might be justified in his observation that “you just [say] the word ‘census’ and people [fall] asleep.”
But the history of the census is a fascinating one. The most infamous debate about the census came immediately upon its creation with the question of how to count the enslaved population. The subsequent three-fifths clause remains one of the most disgraceful mathematical work-arounds in United States history. Other aspects of the census betray a more hopeful history, however. From the very beginning men like Madison and Jefferson were fascinated by their country’s size, scope, and growth and, like good men of the Enlightenment, they wanted such things to be measured scientifically. In debates over the first census Madison suggested that the marshals should not only count people but document their sex and ages so that Congress would know how large an army it could field. Such ideas were tabled for the first census, but gradually the forces of Madisonian curiosity began to win out.
Historian Patricia Cline Cohen has noted that the first half of the nineteenth century witnessed a dramatic expansion in quantification, numeracy, and data-gathering in the United States. The reasons were manifold: a booming capitalist economy incentivized greater standardization; precise measurements and information became invaluable; common schools made the mass of men mathematically literate and the profit motive focused them on the bottom line; and suddenly American newspapers were awash in numbers—prices, tonnages, and times. “Their minds [are] accustomed to definite calculations,” Tocqueville said of the Americans. New money is rarely lazy money, and it is usually money that is good at math. Lincoln is often praised for the lilt of his language and for accomplishing what Garry Wills called a “revolution in style.” But in his early days the sixteenth president was a relentless logician who was as likely to quote Euclid as Shakespeare, and from an early age he was disposed to be mathematically precise about his income and expenses.
To be sure, this growth of numeracy had its less savory side. Herman Melville wrote The Confidence Man in this period. Edgar Allan Poe wrote “Diddling Considered as One of the Exact Sciences.” After a sojourn in the United States, Charles Dickens noted that the Americans’ most “prominent feature” was a “love of ‘smart’ dealing, which gilds over many a swindle and gross breach of trust.”
But if Americans put their calculating minds first to making money, they put them also to the scientific study of the themselves. The 1790 census may have been a straightforward head count, but the maturation of statistical sciences, coupled with the pride and curiosity of a country growing and changing so dramatically, ensured that the census would be constantly fine-tuned and expanded in the decades after. In 1800, the census for the first time collected broad age ranges of the free white population, just as Madison had originally wanted. In the run-up to the 1810 effort, Jefferson suggested collecting Americans’ occupations, marital status, and countries of origin. His notion was defeated (for a time) but with Europe embroiled in the Napoleonic Wars and many Americans curious about their war footing, Congress approved the first census of American manufacturing. Similar adjustments followed as priorities and interests changed. The 1830 census enumerated the number of Americans who were deaf, dumb, or blind. The 1840 census counted the country’s number of war pensioners, schools and colleges, and the number of Americans who were illiterate, idiotic, or insane.
And then came the dramatic (and improbable) expansions of 1850. In 1849, when Congress typically would have debated and authorized the shape of the upcoming census, House members were busy trading body blows (sometimes literally) over the shape of slavery in the territories recently acquired from Mexico. “We dream of negroes, hear nothing else by the wayside or in the House [or] at our meals,” complained one vitriolic legislator. With too little oxygen left for anything else, Congressmen responded typically—on the last day of the session, they authorized the formation of a board to deal with the problem and fled the capitol.
When they returned in 1850, all were surprised (and some were appalled) by all that had been achieved. During the Congressional intercession, Zachary Taylor had appointed Pennsylvanian Joseph C. G. Kennedy to chair the Census Board. A political appointee with few obvious qualifications for office, Kennedy had nevertheless gone earnestly to work, consulting with the heads of the country’s two major statistical societies and formulating a questionnaire more ambitious than any seen before. Where all prior censuses had understood the constituent unit of the American polity as the household, Kennedy’s questionnaire would gather data on individuals—men and women, adults and children, the free and the enslaved. Schedule One would tabulate the name, address, age, sex, color, occupation, place of birth, and marital status of every free American, asking them whether they had attended school within the year, whether they were deaf, dumb, blind, insane, idiotic, or a pauper, and whether they owned any real estate, and if so, how much. Schedule Two would document each slave’s name, age, sex, color, and place of birth, along with whether they were deaf, dumb, blind, insane, idiotic, or a fugitive, and, in the case of women, how many children they had borne and whether those children were living or dead. Schedule Three would ask a separate battery of questions about anyone who had died on the property in the preceding year. Schedules Four and Five would focus on Agriculture and Manufacturing, and Schedule Six would seek to pull together social statistics about taxes, schools, newspapers, pauperism, crime, wages, religion, and libraries. Confident in his work, sure of his authority, and worried about his deadlines (the census was supposed to be taken over a one-month period in the summer), Kennedy had crafted his blank forms and sent them to the printer for duplication.
By the time Congress reconvened, then, Kennedy had achieved such a dramatic expansion of the census that legislators had a difficult time gutting it all, although they certainly did their best. As might be guessed, Schedule Two drew the lion’s share of the scrutiny. In previous censuses, slaves had been treated essentially as property attached to the household. A male head of house, for instance, might be listed as having four male slaves between the ages of ten and twenty; three female slaves between the ages of forty and fifty; and two slave children under the age of ten. Kennedy’s questionnaire, by contrast, would actually name the slaves and then ask about their children and families. Grilled by Congress, Kennedy claimed that these adjustments were designed solely to ensure greater accuracy; a census marshal would be less prone to error if he could use the slaves’ names as a check against over- or under-counting. But Congressmen North and South instantly seized on the potential implications of the data he sought to gather. Senator Andrew Butler of South Carolina, for instance, demanded that no slave names should be recorded, an objection which quickly passed. Senator William King of Alabama then demanded that no data should be gathered on where the slaves had been born, which passed also. Such data would today be invaluable. African Americans tracing their ancestry would have ancestors’ names to go by. With a sense of slaves’ (forced) movements, historians would have a much better sense of the scale, scope, and timing of the interstate slave trade, the sale of a million men, women, and children 'down the river’ to satisfy the labor demands of King Cotton.
But whatever they told themselves about the 'positive good’ of slavery, southern Congressmen seemed a little skittish about what Kennedy’s statistics might reveal. The proposed question about slave children, for instance, drew instant fire; census marshals would be potentially drawn into questions about race-mixing (and whose mulatto children were whose) and about the possibility of higher infant mortality rates among the enslaved. Congressman William King tried to treat this all as a joke. There was no point in asking such questions, he noted, because in his experience “the [slave] woman herself, in nine out of ten cases, when she has had ten or fifteen children, does not know how many she has actually had.” This amused most of his Senate colleagues, but to his credit, the abolitionist William Seward did not get the joke. “There is no woman,” he said, “with great deference to the Senator from Alabama, who can have forgotten the number of children that she has borne.... I wish to know also what is the extent of the education or of instruction that prevails [among the enslaved], so as to ascertain whether they are advancing toward that better condition which constitutes, the only excuse, as I understand, that we have for holding them in servitude.” Seward was pilloried for his inflammatory remarks, and Senator Underwood of Kentucky tried to pacify things by noting that infant mortality data could be useful for the burgeoning southern business of slave life insurance, but it was all to no avail. Schedule Two was effectively gutted by Congress, and Kennedy was ordered to cancel his contract with the printer and prepare new forms.
What had apparently escaped Congressional attention, however, was Schedule Three, and thus was the Mortality Census born, the strange child of the precise attention of statisticians and the lax oversight of Congress.
Before we can turn to the data, we must understand the process and context of its collection. All census marshals were instructed to complete the work of Schedules One and Two and then ask if any member of the household had died during the previous year—specifically between the dates of June 1, 1849 and May 31, 1850. If so, he then asked the name, age, sex, color, occupation, status (free or slave), marital status, and place of birth of the deceased as well as the cause of death and the duration of the illness, if applicable.
There are myriad problems with this approach. First, one can imagine that many marshals were, by Schedule Three, chafing to move on to the next household and not particularly keen to discuss the health histories of the recently deceased with the still grieving. The hoi polloi of the antebellum backwoods didn’t like strangers and liked strangers asking questions even less; to them the census takers were the vanguard of the taxmen. “We escaped without any drubbings,” said one marshal of his experience, but “we came unpleasantly near catching a dozen.”
Even if the marshals were up to the task of cross-questioning the recently bereaved, family members might have had innumerable reasons to withhold complete and accurate information. What farmer of the period would be comfortable telling a perfect stranger that his unwed daughter had died in childbirth just last month? Given such circumstances, under-reporting on the Mortality Census was certainly significant and perhaps even massive. Then again, folks were equally likely to give too much information—and more than a few individuals were recorded as having died of menstruation, masturbation, herpes, and other unlikely scenarios.
This raises a third problem with the Mortality Census. It tasked people not remotely versed in medicine to pronounce a cause of death. This problem the Census Bureau had thought of, though by the time the bureau began dealing with it, Kennedy had been sacked.
Competent and enthusiastic, Kennedy had nevertheless been a political appointee, and he should not have been surprised when a new president appointed a new superintendent for the census. Elected in 1852, Franklin Pierce was a Democrat, where Taylor had been a Whig, and when the White House changes parties the high number of people to be patronized and punished means the turnover runs deep.
Given the Democrats strong base in the south, the choice of James D. B. DeBow was quite shrewd. Living in New Orleans, DeBow was famous across the south as the editor and writer of DeBow’s Review. “Just as a homeowner today might subscribe to a magazine like This Old House,” Ta-Nehisi Coates has written, “slaveholders had journals such as De Bow’s Review, which recommended the best practices for wringing profits from slaves.” Making the case for slave reparations, Coates was exaggerating for effect but not much. DeBow was a sophisticated statistician and demographer, however, well-versed in tabulating data. In this sense, he was better qualified than Kennedy, and in 1853 he relocated to Washington, D.C. to begin preparing the 1850 census for final publication.
Kennedy had left the office in good shape, but DeBow felt nevertheless compelled to put his stamp on the place and reorganizing the staff and developing new workflows took time. Thus when DeBow got around to the headaches inherent in the mortality data, he was behind schedule and thoroughly worn down. Hunched over tiny type for months of long hours, he seemed almost wistful in introducing America to its first Mortality Census:
“It is more easy to satisfy mankind of the value of any other branch of statistics than that which relates to the numbers that die in any given period, their ages, their sex, occupation, condition and nativity, and the causes which produce such deaths. The consequence is that the facts remain uncollected or unrecorded, while everybody seems busy enough, more especially in our practical, money-making country, in running after those which relate to the fluctuations of stocks, the valuation of exports and imports, the rates of taxation and the results in agriculture and manufactures, internal improvements and general commerce. The life of man is of less importance than his larder and his cloth. It was the remark of a physician, now no more, founded on severe experience, that the lawyer who saved the property of his client was always quicker, better and more cheerfully paid than the doctor who saved his life. Steamboat and railroad companies understand this well enough, for whilst they must pay heavily for destroying a bundle of merchandise, in human life they can and do wanton at pleasure. Such being the case, it is not singular that investigations having for their object sanitary improvement are pursued slower and later in all countries than those which relate to property. They meet with greater impediments and their results are least consulted or credited. man is the same in all ages, and this fact meets us in all.”
DeBow struck a similarly ambivalent tone throughout the volume. Flattering the legislators, and to some degree throwing his predecessor to the political wolves, he noted that “had there been as much care observed in the execution of the law” (the collecting of the data) as there had been in framing the law and preparing the data “a mass of information must have resulted relating to the sanitary condition of the country attained as yet in no other part of the world. This, however, would have been expecting too much.” Instead, DeBow was forced to admit that he had no illusions about the quality or completeness of his data. He guessed that “in the Union at large at least one-fourth of the whole number of deaths have not been reported at all.” He was sure that the rural population had been better counted than the urban and that the older states were better enumerated than the newer. Worse he worried that any attempt to make regional and state comparisons would only be to compare the relative effectiveness of their respective state marshals. Did fewer people die in Mississippi, or did Mississippi do a poorer job of recording deaths? Finally, he worried about relying on self-reported data. Among the educated, he said, the claimed causes of death “may be considered sufficiently near the truth for popular purposes, though falling far short of the precision necessary in skillful scientific calculations.” And among the masses “vagueness and inaccuracy may naturally be expected, even where the parties are disposed to speak the truth and make the best effort to do so.”
Given such official hand-wringing, it is not surprising that demographers have eschewed the mortality census as a collection of “bad data.” Bad data can be good data, however, if you ask the right questions. The self-reported nature of the data, for instance, makes it “bad” if you are interested in a definitive set of medical diagnoses but “good” if you are interested in what common people thought they were dying of. (Surely if a woman thought her son died of masturbation it reveals something about her worldview, her attitude toward her son, and probably her attitude toward masturbation.) Equally fascinating is the process by which the census board disciplined these “vernacular mortalities” into something “scientific.” Working with physicians, DeBow first took the vast catalogue of self-reported causes of death and disciplined them down to a list of 148. This was primarily done by combining cases that were referred to by synonymous popular names. DeBow then sent this “translated and condensed catalogue” to Edward Jarvis, a Harvard trained physician who was beginning to make a national reputation for studying and promoting the value of vital statistics. Jarvis seemed somewhat peeved that the list had already been massaged, and he urged that in future years the census board create a national network of local physicians who could translate vernacular disease names common in their region into something more useful. Nevertheless Jarvis went to work, consulting the nation’s leading nosologists (those who study the classification of diseases), and further winnowed DeBow’s list down to 114. This he did by eliminating some categories and broadening others. Chicken pox, diseases of the eyes, herpes, hives, mumps, ringworm, tetter, and a host of others were simply not fatal. Some of these cases could be recategorized—the chicken pox cases were probably smallpox cases and could be filed under “diseases of the skin.” In other instances, however, the claimed diagnoses were so epiphenomenal to whatever really did the killing that the cases would have to be listed as “unknown.” (Jarvis was on the fence about masturbation. “Onanism,” he said, “possibly, but not probably, was a cause of death. It wastes life and produces other disorders [but] cases under this head should be put under the unknown.”)
From screw-threads to railroad gauges to currency, standardization was both product and producer of America’s burgeoning capitalist economy, and in disciplining Death itself to bureaucratic categories, Jarvis and company were following the tenor of the times. In the process, they laid the foundation for both the American public health system and the assumption that government is responsible for that system. The benefits that have accrued are so numerous that it is perhaps not worth lamenting the consequent demise of vernacular understandings nor the downsides of what Foucault called the state’s “biopower”—its effective tendency to control our bodies even as it cares for them. Jarvis and DeBow knew only that they had struck a blow for the public good. “There never has been, and there may not be again,” Jarvis wrote to DeBow, “another opportunity, such as you now enjoy, of showing to the world the ... names of diseases which are found in the several States and thought to be fatal.” For his part, DeBow also believed that something miraculous had been achieved, in spite of all the problems. Here was a scale of death never before documented so precisely; here was Death aggregated and disciplined into neat little columns. Here were “one-third of a million people scattered over three millions of square miles of territory,” all making their varied ways to the grave in a single year. “The value of such a multitude of facts cannot but be very great, even although they do not constitute the whole of them,” DeBow concluded. “We are every day accustomed to draw deductions for the whole from a part, and to argue out the true and complete from the approximate and uncertain.”
Taken each decade from 1850 to 1890, the mortality census grew in sophistication even as it culminated in, and was replaced by, the Bureau of Vital Statistics and the formalization of death certificates at the turn of the century. The story of that evolution is a fascinating one, but the more immediate question is whether the 1850 mortality census can help put the records of the coroner’s office into a broader context of death and dying in the nineteenth-century South.
Drawing Deductions from the Approximate and Uncertain
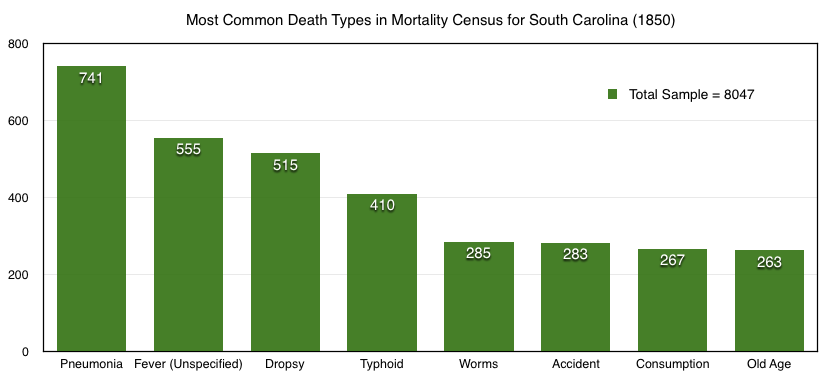
The 1850 mortality census recorded 8,047 deaths in South Carolina for the year beginning June 1, 1849, a crude mortality rate of 12 people per thousand. While undoubtedly an undercount, as DeBow had noted, this number is relatively higher than we see in the current United States, which has a crude mortality rate of only 8.1 people per thousand despite a much older population. This discrepancy is a measure of the degree to which improvements in modern medicine, public health, labor and living conditions have all succeeded in ameliorating and even eradicating some causes of death.
Still, we have to be careful. DeBow and Jarvis had shaken their heads at the pitiful diagnoses of the plebes, but their own “scientific” approach was riddled with assumptions—nowhere more clearly than on the subject of race. African Americans (the vast majority of them enslaved) made up 57% of South Carolina’s population but 65% of the mortality cases. This much could be explained; their work routines, diets, accommodations, and access to health care might all have contributed to higher mortalities. What boggles the mind, however, is what they supposedly died of:
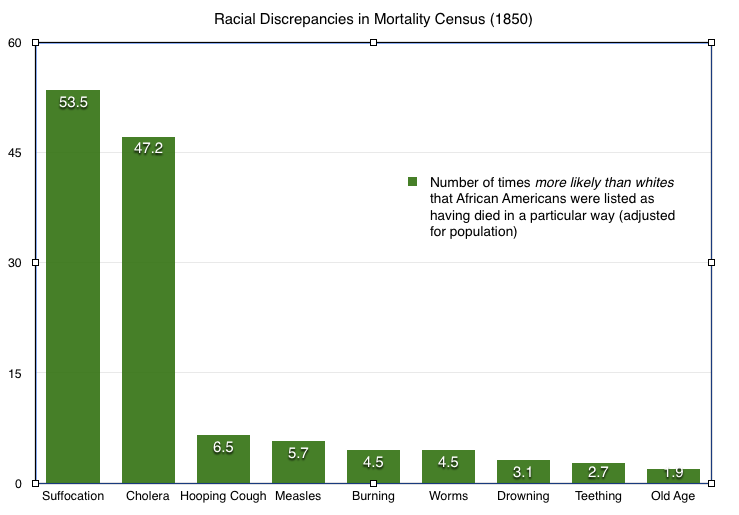
According to the mortality census, African Americans were 53.5 times more likely to die of suffocation than whites. They were 47.2 times more likely to die of cholera—almost five times more likely to die of worms or of burning. What is to be made of such discrepancies? The ‘suffocation’ deaths have long been discredited. At the time, planters and physicians believed that careless slave mothers were rolling over their infants in their sleep, thereby suffocating them. Most of these cases were crib death or SIDS, news that might have come as cold comfort to the enslaved mothers who were told that they had, purposely or not, killed their own children. The ‘cholera’ deaths are likewise baffling until we note the one disease that disproportionately affected whites—yellow fever. In the racist understanding of black biology, African Americans were “habituated, from infancy, to the combined impression of atmospheric heat and miasma” and thereby enjoyed a “general exemption from bilious and hepatic diseases” like yellow fever. This scientific mumbo-jumbo may explain why so many African Americans died of ‘cholera’—because they were not ‘allowed’ to die of yellow fever. Once again, we find ourselves asea in good/bad data. Like the self-reported assessments on which they were based, the ‘scientific’ categorizations of the mortality census are simultaneously a deeply flawed index of nineteenth-century mortality and a deeply informative index of nineteenth-century blindspots and assumptions. Some of the categories, like suffocation and cholera, are so flawed in one way that they become useful in another—fair indicators of the ‘sciencing’ of race. African Americans were not twice as likely to die of old age, for example; whites were simply more likely to attribute black death to a body that just ‘gave out.’ In other categories, however, we can imagine that the mortality census captured medical truths as well. African Americans probably were more likely to be burned or to drown, for instance. Diagnosis in such cases is relatively straightforward, and these are the sorts of deaths the coroner would investigate.
Of the 8,047 deaths listed in the South Carolina mortality census, something like 382, or five percent, would have qualified as ‘suspicious or sudden,’ thus triggering an investigation by the coroner. This would include the stillbirth and suffocation deaths, the suicides, murders, and accidents. We will never know how many of these cases were actually investigated because a complete set of coroner’s inquests for all South Carolina counties does not exist. It is vaguely possible that coroners investigated more than these—cases that may have seemed suspicious at the time but proved ordinary upon inquest—but it is equally possible that coroners ignored or never learned about cases well within their purview. Three hundred and fifteen people were recorded as having died in Edgefield County between June 1, 1849 and May 1, 1850—a number we know to be an undercount. In that same period, Edgefield’s coroners investigated exactly eleven cases, or roughly three percent. (Some inquests could have been lost, but because Edgefield’s inquests for this period were copied into a single bound notebook, we can be more confident that we have a full run.) This three percent number is probably as good an approximation as we are likely to get, which means that ninety-seven percent of the time, when people died the coroner did nothing. CSI:D is devoted to the other three percent, the times when the coroner did something.
NEXT: Acts: Homicide
Mortality Census for South Carolina in 1850
| Death Type | Whites | African Americans | Total | ||||
|---|---|---|---|---|---|---|---|
| Men | Women | Total | Men | Women | Total | ||
| abscess | 0 | 1 | 1 | 2 | 1 | 3 | 4 |
| accident (unspecified) | 39 | 10 | 49 | 56 | 23 | 79 | 128 |
| accident (burned) | 4 | 10 | 14 | 30 | 61 | 91 | 105 |
| accident (drowned) | 7 | 0 | 7 | 30 | 4 | 34 | 41 |
| accident (scalded) | 1 | 0 | 1 | 1 | 0 | 1 | 2 |
| accident (shot) | 4 | 0 | 4 | 2 | 1 | 3 | 7 |
| amputation | 0 | 0 | 0 | 2 | 0 | 2 | 2 |
| apoplexy | 20 | 10 | 30 | 15 | 18 | 33 | 63 |
| asthma | 5 | 3 | 8 | 11 | 6 | 17 | 25 |
| bowels, disease of | 13 | 11 | 24 | 21 | 12 | 33 | 57 |
| brain, disease of | 1 | 2 | 3 | 3 | 2 | 5 | 8 |
| bronchitis | 6 | 5 | 11 | 10 | 6 | 16 | 27 |
| cancer | 6 | 13 | 19 | 5 | 10 | 15 | 34 |
| carbuncle | 0 | 2 | 2 | 0 | 0 | 0 | 2 |
| catarrh | 12 | 13 | 25 | 38 | 58 | 96 | 121 |
| childbirth | 0 | 48 | 48 | 0 | 70 | 70 | 118 |
| chlirosis | 0 | 0 | 0 | 0 | 1 | 1 | 1 |
| cholera | 1 | 0 | 1 | 39 | 29 | 68 | 69 |
| cholera (infantum) | 15 | 13 | 28 | 16 | 20 | 36 | 64 |
| cholera (morbus) | 5 | 4 | 9 | 8 | 5 | 13 | 22 |
| colic | 9 | 8 | 17 | 19 | 15 | 34 | 51 |
| congestion | 1 | 5 | 6 | 2 | 2 | 4 | 10 |
| congestion (bowels) | 1 | 2 | 3 | 3 | 5 | 8 | 11 |
| congestion (brain) | 6 | 11 | 17 | 13 | 8 | 21 | 38 |
| congestion (lungs) | 0 | 0 | 0 | 0 | 2 | 2 | 2 |
| consumption | 52 | 75 | 127 | 60 | 80 | 140 | 267 |
| convulsions | 19 | 20 | 39 | 51 | 63 | 114 | 153 |
| croup | 34 | 25 | 59 | 72 | 71 | 143 | 202 |
| debility | 0 | 0 | 0 | 0 | 2 | 2 | 2 |
| diabetes | 3 | 0 | 3 | 0 | 0 | 0 | 3 |
| diarrhea | 20 | 16 | 36 | 42 | 51 | 93 | 129 |
| dirt eating | 1 | 0 | 1 | 4 | 3 | 7 | 8 |
| dropsy | 110 | 70 | 180 | 168 | 167 | 335 | 515 |
| dysentery | 22 | 14 | 36 | 33 | 18 | 51 | 87 |
| dyspepsia | 8 | 6 | 14 | 1 | 4 | 5 | 19 |
| epilepsy | 0 | 3 | 3 | 5 | 5 | 10 | 13 |
| erysipelas | 3 | 4 | 7 | 2 | 3 | 5 | 12 |
| executed | 0 | 0 | 0 | 3 | 0 | 3 | 3 |
| fever (unspecified) | 133 | 111 | 244 | 136 | 175 | 311 | 555 |
| fever (bilious) | 49 | 63 | 112 | 78 | 83 | 161 | 273 |
| fever (brain) | 7 | 0 | 7 | 5 | 3 | 8 | 15 |
| fever (congestive) | 42 | 38 | 80 | 35 | 38 | 73 | 153 |
| fever (inflammatory) | 2 | 1 | 3 | 0 | 1 | 1 | 4 |
| fever (intermittent) | 9 | 4 | 13 | 6 | 10 | 16 | 29 |
| fever (puerperal) | 0 | 7 | 7 | 0 | 13 | 13 | 20 |
| fever (remittent) | 1 | 0 | 1 | 5 | 2 | 7 | 8 |
| fever (scarlet) | 18 | 19 | 37 | 24 | 14 | 38 | 75 |
| fever (typhoid) | 102 | 65 | 167 | 133 | 110 | 243 | 410 |
| fever (yellow) | 80 | 39 | 119 | 2 | 3 | 5 | 124 |
| gravel | 4 | 0 | 4 | 5 | 0 | 5 | 9 |
| head, disease of | 2 | 0 | 2 | 6 | 4 | 10 | 12 |
| heart, disease of | 8 | 8 | 16 | 8 | 6 | 14 | 30 |
| hemorrhage | 7 | 1 | 8 | 7 | 3 | 10 | 18 |
| hernia | 1 | 0 | 1 | 8 | 2 | 10 | 11 |
| hives | 16 | 10 | 26 | 8 | 8 | 16 | 42 |
| hooping cough | 20 | 6 | 26 | 115 | 128 | 243 | 260 |
| hydrocephalus | 0 | 1 | 1 | 3 | 3 | 6 | 7 |
| inflammation | 13 | 10 | 23 | 9 | 10 | 19 | 42 |
| inflammation (bowels) | 22 | 13 | 35 | 18 | 12 | 30 | 65 |
| inflammation (brain) | 10 | 16 | 26 | 13 | 9 | 22 | 48 |
| inflammation (stomach) | 2 | 3 | 5 | 3 | 0 | 3 | 8 |
| insanity | 3 | 1 | 4 | 0 | 1 | 1 | 5 |
| intemperance | 3 | 0 | 3 | 0 | 0 | 0 | 3 |
| jaundice | 1 | 5 | 6 | 1 | 1 | 2 | 8 |
| kidneys, disease of | 2 | 0 | 2 | 0 | 1 | 1 | 3 |
| killed | 2 | 0 | 2 | 7 | 0 | 7 | 9 |
| leprosy | 0 | 0 | 0 | 0 | 1 | 1 | 1 |
| lightning | 0 | 1 | 1 | 6 | 3 | 9 | 10 |
| liver, disease of | 22 | 18 | 40 | 9 | 11 | 20 | 60 |
| lockjaw | 2 | 0 | 2 | 10 | 8 | 18 | 20 |
| lungs, disease of | 2 | 2 | 4 | 6 | 10 | 16 | 20 |
| malformation | 1 | 0 | 1 | 2 | 3 | 5 | 6 |
| mania-a-potu | 5 | 0 | 5 | 0 | 0 | 0 | 5 |
| marasmus | 1 | 3 | 4 | 3 | 7 | 10 | 14 |
| measles | 2 | 5 | 7 | 29 | 33 | 62 | 69 |
| menses, excess of | 0 | 0 | 0 | 0 | 3 | 3 | 3 |
| menses, suppression of | 0 | 0 | 0 | 0 | 2 | 2 | 2 |
| mortification | 1 | 0 | 1 | 1 | 2 | 3 | 4 |
| mumps | 0 | 0 | 0 | 0 | 1 | 1 | 1 |
| murder | 5 | 0 | 5 | 1 | 0 | 1 | 6 |
| neuralgia | 5 | 1 | 6 | 0 | 2 | 2 | 8 |
| old age | 22 | 48 | 70 | 111 | 82 | 193 | 263 |
| paralysis | 26 | 18 | 44 | 12 | 13 | 25 | 69 |
| piles | 0 | 0 | 0 | 3 | 0 | 3 | 3 |
| pleurisy | 5 | 6 | 11 | 14 | 13 | 27 | 38 |
| pneumonia | 147 | 90 | 237 | 290 | 214 | 504 | 741 |
| poison | 1 | 0 | 1 | 4 | 2 | 6 | 7 |
| putrid sore throat | 8 | 10 | 18 | 0 | 1 | 1 | 19 |
| quinsy | 15 | 10 | 25 | 9 | 5 | 14 | 39 |
| rheumatism | 10 | 4 | 14 | 8 | 9 | 17 | 31 |
| rickets | 1 | 0 | 1 | 1 | 0 | 1 | 2 |
| scrofula | 1 | 2 | 3 | 13 | 12 | 25 | 28 |
| scurvy | 0 | 0 | 0 | 0 | 1 | 1 | 1 |
| spine, disease of | 4 | 1 | 5 | 5 | 3 | 8 | 13 |
| stillborn | 4 | 2 | 6 | 3 | 2 | 5 | 11 |
| stomach, disease of | 0 | 0 | 0 | 2 | 1 | 3 | 3 |
| suffocation | 1 | 0 | 1 | 42 | 35 | 77 | 78 |
| suicide | 1 | 2 | 3 | 1 | 0 | 0 | 4 |
| teething | 18 | 16 | 34 | 66 | 66 | 132 | 166 |
| tetanus | 0 | 0 | 0 | 2 | 0 | 2 | 2 |
| throat, disease of | 14 | 18 | 32 | 17 | 14 | 31 | 63 |
| thrush | 2 | 0 | 2 | 9 | 7 | 16 | 18 |
| tumor | 1 | 3 | 4 | 2 | 2 | 4 | 8 |
| ulcer | 4 | 0 | 4 | 6 | 2 | 8 | 12 |
| uterus, disease of | 0 | 2 | 2 | 0 | 5 | 5 | 7 |
| venereal | 5 | 0 | 5 | 2 | 5 | 7 | 12 |
| white swelling | 1 | 0 | 1 | 2 | 0 | 2 | 3 |
| worms | 18 | 20 | 38 | 132 | 115 | 247 | 285 |
| unknown | 202 | 158 | 360 | 441 | 411 | 852 | 1212 |